UltraScan™ 650 bone densitometer

Device Description:
The UltraScan 650 is a bone sonometer that is designed to non-invasively and quantitatively assess the amount of bone at the 1/3 location of the radius in the forearm of an individual. The UltraScan 650, with a user-supplied laptop, is designed for the measurement of bone mineral density (BMD in g/cm2) of the radius at the 1/3 location. The UltraScan 650 outputs a BMDUS Index an estimate of the BMD that would be measured by dual-energy X-ray absorptiometry (DXA) at the same anatomical location, that is, an estimate of BMDDXA, at the 1/3 radius. The UltraScan 650 also outputs the T-score in standard deviations (SD) and Z-score in SD as well. The precision of the measurement is 2.1%, when expressed as a coefficient of variation.
Indications for Use:
UltraScan 650 can be used to determine BMDUS Index in adult men and women and to assess appendicular fracture risk in postmenopausal women.
The BMDUS is a clinical measure based on ultrasound variables of the forearm which is highly correlated with the value of BMD of the 1/3 radius as provided by DXA, with a standard error of the estimate of 0.041 grams/cm2.
BMDUS is expressed in grams/cm2 and as a T- and z-score, derived from comparison to a normative x-ray absorptiometry reference database.
BMDUS has a precision comparable to that of x-ray absorptiometry, which makes it suitable for monitoring bone changes in postmenopausal women.
The UltraScan™ 650 Forearm Scanner is an ultrasound based device designed to quantitatively assess the radius bone at the 1/3rd location. This site has been measured with x-rays for decades and has been shown to be an excellent proxy for fracture risk. The UltraScan™ 650 makes each radiation-free measurement in less than ten (10) seconds. The UltraScan™ 650 should allow for much wider diagnosis and detection of individuals at risk of osteoporotic fracture.
Summary of Test Data:
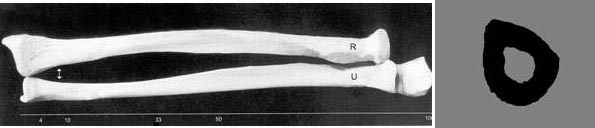
(A comprehensive paper summarizing the performance of the UltraScan 650 can be found in our publication by Stein et al. in Ultrasound in Medicine & Biology.)The UltraScan™ 650 is a through-transmission system that has a linear array 64 element receiver with a single element source, operating at 3.5 MHz. The system is designed to measure the radius at the 1/3rd location (shown as the radius and ulna and the cross-section of the radius in the pictures below), a site that has been measured for decades with x-ray densitometers.
Data from both simulations and in vitro experiments have provided strong evidence that the UltraScan™ 650 can estimate bone mass clinically. Please see the two papers available on our web site, which provide full details on the experiments: "Ultrasound Simulation in Bone" and "Ultrasonic Assessment of the Radius in vitro". Some of the results of these two papers are summarized here.
Using CyberLogic's software packages for ultrasound simulation (Wave2000®), we have shown how the Net Time Delay (NTD) technology (U.S.,China and India Patents) that is incorporated in the UltraScan™ 650 enables the bone mass, as represented by cortical thickness and cortical cross-sectional area, to be accurately estimated.
For example, the figure below shows simulation results on twenty (20) human radial cross-sectional images. As may be seen, there is excellent correspondence between the NTD and cortical thickness (this data has an R-squared value of 0.98).

The figure below shows the correlation obtained in simulations between the cortical cross-sectional area (CSA) at the same 1/3rd location of the radius, with an ultrasound based estimate at the same site. The ultrasound based estimate uses a non-linear combination of two distinct NTD parameters; please see the papers referred to above for technical details. Note that the cortical CSA is generally proportional to the bone mineral content in grams measured with dual-energy x-ray absorptiometry (DXA). This data has an R-squared value of 0.88.
As noted above, in vitro experiments have also been carried out. The same 20 radial bones were ultrasonically interrogated with a laboratory prototype of the UltraScan™ 650. The two figures below show the analogous data for cortical thickness (denoted as "Bone Thickness") and cortical cross-sectional area (denoted as "CSA") of the radius at the 1/3rd location. Experiments were carried out in a water tank.
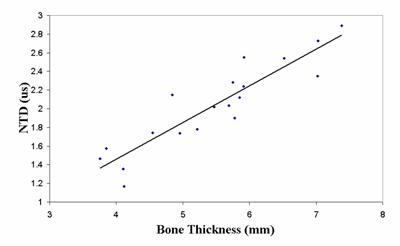
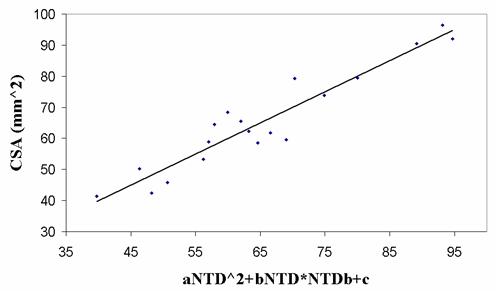
As may be seen, there is good correspondence between the ultrasound and bone mass data, with R-squared values of 0.83 for cortical thickness and 0.90 for cortical cross-sectional area.
A clinical study was recently completed using the UltraScan™ 650 that studied the differences in cortical cross-sectional area for the dominant and non-dominant arms (radii). Please see the abstract presented at the 31st meeting of the American Society for Bone and Mineral Research, September 11-15, 2009, in Denver Colorado, which is available on CyberLogic's website, "Effect of Arm Dominance on Quantitative Transmission Ultrasound at the Forearm". Briefly twenty-one (21) people were evaluated with the UltraScan™ 650, each being measured 3 times on both the left and right arms and arm dominance recorded. Ambidextrous individuals were excluded from the study. A paired one-sided t-test was used to evaluate the statistical difference between dominant and non-dominant arms, and short term precision (%RMS-CV) was also computed.
The data (see the bar graph below) showed that the dominant arms had 5.8% more cortical cross-sectional area, although there was a relatively high degree of variability (in 7 of the 21 subjects the non-dominant arm had a larger CCSA) and the P-value was equal to 0.17.
The results obtained are consistent with prior studies using DXA that showed a 6-9% increase in bone mineral content (BMC) in the dominant vs. non-dominant arms (see for example the book by Bonnick SLB, Bone Densitometry in Clinical Practice , published in 2004 by Humana Press in Totowa, NJ). This suggests that the ultrasound estimate of CCSA and x-ray determined BMC may be closely related.
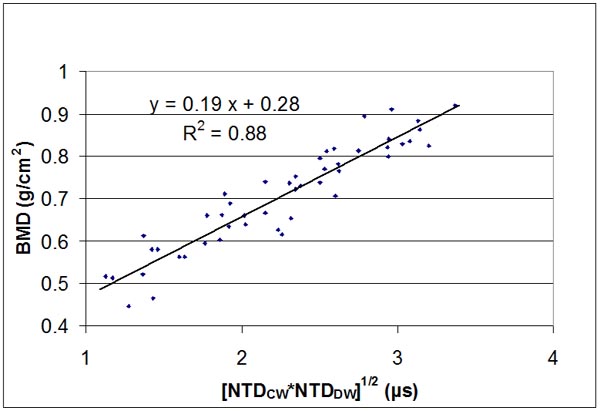
In a clinical study, forty-nine adult subjects were recruited for this study at Columbia University under an IRB approved protocol. Each subject was measured at the 1/3rd radius with the UltraScan 650. For each subject radial bone density at the same 1/3rd location was determined using DXA. For this clinical data, plots showing the relationships of [NTDCW*NTDDW]1/2 vs BMD, together with a linear regression curve fit, are shown in figure above. The linear correlation between them was r = 0.94. In the figure, the parameter [NTDCW*NTDDW]1/2 was determined ultrasonically with the UltraScan 650 and BMD was measured using DXA.